

MRD
response rate
90%
(n=44/49)
BLINCYTO® (blinatumomab) is indicated for the treatment of CD19-positive B-cell precursor acute lymphoblastic leukemia (ALL) in first or second complete remission with minimal residual disease (MRD) greater than or equal to 0.1% in adult and pediatric patients. ... Read More

MT103-205, the pivotal study of BLINCYTO® in pediatric patients with R/R B-cell precursor ALL: International, open-label, single-arm, phase 1/2 study of single-agent BLINCYTO® in 70 patients < 18 years of age with B-cell precursor ALL and > 25% BM blasts who were primary refractory, in first relapse after full salvage induction, in second or later relapse, or in any relapse after HSCT. Primary endpoint was CR/CRh* in first 2 cycles: 33% (n=23/70); (95% CI: 22.1-45.1).1,2,†
Learn more about the MT103-205 pivotal study
†CR was defined as ≤ 5% of blasts in the BM, no evidence of circulating blasts or extramedullary disease, and full recovery of peripheral blood counts (platelets > 100,000/microliter and ANC > 1,000/microliter). CRh* was defined as ≤ 5% of blasts in the BM, no evidence of circulating blasts or extramedullary disease, and partial recovery of peripheral blood counts (platelets > 50,000/microliter and ANC > 500/microliter).1
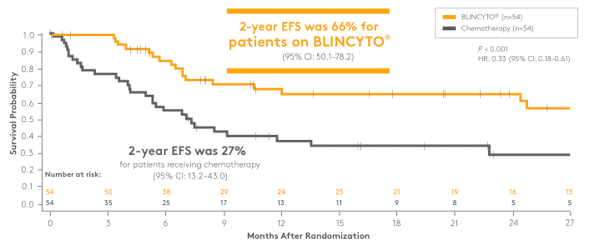
Study design: a randomized, controlled, open-label, phase 3 study of BLINCYTO® vs chemotherapy as post-reinduction consolidation therapy prior to HSCT in 108 pediatric patients > 28 days and < 18 years of age with Ph(–) B-cell precursor ALL in high-risk first relapse.* After receiving reinduction chemotherapy followed by 2 blocks of high-risk consolidation chemotherapy,† patients were randomized to receive one cycle of BLINCYTO® (n=54) or a third block of high-risk consolidation chemotherapy (n=54).‡ Primary endpoint was EFS: 66% at 2 years for patients on BLINCYTO® (n=54) vs 27% for patients receiving chemotherapy (n=54); P < 0.001; HR: 0.33 (95% CI: 0.18–0.61). Selected secondary endpoints: OS, incidence of relapse, MRD response, incidence of AEs.3
*High risk was defined as very early or early iBM relapse, very early combined BM + EM relapse, or very early iEM relapse. Very early relapse was defined as < 18 months after primary diagnosis, and early relapse was defined as ≥ 18 months after primary diagnosis and < 6 months after completion of primary therapy.4
†Induction therapy and cycles of HC1 and HC2 chemotherapy administered according to the IntReALL HR 2010, ALL-REZ BFM 2002, ALL R3, COOPRALL, and AIEOP ALL REC 2003 protocols.3
‡Third block of consolidation chemotherapy, HC3, included: dexamethasone IV/vincristine IV/daunorubicin IV/methotrexate IV/ifosfamide IV/PEG-asparaginase IV/IM.3
EFS for BLINCYTO® vs chemotherapy3
Patients who did not achieve remission or died before assessment were assigned one day of event-free survival. Patients alive and event free were censored on their last assessment date.
AE, adverse event; EFS, event-free survival; EM, extramedullary; HC1, high-risk consolidation block 1; HC2, high-risk consolidation block 2; HC3, high-risk consolidation block 3; HR, hazard ratio;
iBM, isolated bone marrow; iEM, isolated extramedullary; IM, intramuscular; MRD, measurable or minimal residual disease; OS, overall survival; Ph(–), Philadelphia chromosome-negative.
MRD
response rate
90%
(n=44/49)
of patients who received BLINCYTO® achieved MRD negativity* vs 54% (n=26/48) of patients who received chemotherapy3
*MRD < 10–4, evaluated in a central laboratory by PCR.3
PCR, polymerase chain reaction.
| Key inclusion criteria3 |
|---|
| High-risk B-cell precursor ALL in first relapse |
| < 5% blasts or between 5%–25% blasts in BM |
| Key exclusion criteria3 |
| Clinically relevant CNS pathology requiring treatment |
| Evidence of current CNS (CNS2, CNS3) involvement by ALL§ |
| Abnormal renal or hepatic function prior to start of treatment |
*High risk was defined as very early or early iBM relapse, very early combined BM + EM relapse, or very early iEM relapse. Very early relapse was defined as < 18 months after primary diagnosis, and early relapse was defined as ≥ 18 months after primary diagnosis and < 6 months after completion of primary therapy.4
†Induction therapy and cycles of HC1 and HC2 chemotherapy, administered according to the IntReALL HR 2010, ALL-REZ BFM 2002, ALL R3, COOPRALL, and AIEOP ALL REC 2003 protocols.3
‡Third block of consolidation chemotherapy, HC3, included: dexamethasone IV/vincristine IV/daunorubicin IV/methotrexate IV/ifosfamide IV/PEG-asparaginase IV/IM.3
§CNS2, patients with WBC count in CSF < 5 per microliter and having blasts in the CSF; CNS3, patients with WBC count in CSF ≥ 5 per microliter and having blasts in the CSF.5
**One patient in the blinatumomab group with IAMP21 and one patient in the consolidation chemotherapy group with t(17;19)(q22;p13)/TCF3-HLF also carried a genetic abnormality predicting an unfavorable prognosis.3
CSF, cerebrospinal fluid; WBC, white blood cell.
See the full safety profile of the Amgen 20120215 study
Learn moreStudy design: a randomized, controlled, open-label, phase 3 study of 208 patients 1–27 years of age with Ph(–) B-cell precursor ALL in high-risk* or intermediate-risk first relapse of B-cell precursor ALL.†,‡ Following one UKALLR3 reinduction chemotherapy block, patients in the high-risk and intermediate-risk groups were randomized to receive cycles 1 and 2 of BLINCYTO® (n=105) as post-reinduction consolidation therapy or blocks 2 and 3 of chemotherapy consolidation (n=103) based on the UKALLR3 trial.§ The primary endpoint was DFS: 54% at 2 years for patients receiving BLINCYTO® (n=105) vs 39% for patients receiving chemotherapy (n=103); P = 0.03; HR: 0.70 (95% CI: 0.47–1.03). Secondary endpoint: OS, exploratory endpoint: MRD response, post hoc endpoint: ability to proceed to HSCT.5
*Patients who had an iBM or combined BM + EM relapse < 36 months or who had an iEM relapse < 18 months were assigned to the high-risk group.5
†Patients who had an iBM or combined BM + EM relapse ≥ 36 months or who had an iEM relapse ≥ 18 months and MRD ≥ 0.1% at end of induction were assigned to the intermediate-risk group.5
‡A low-risk randomization arm was also part of the study.5
§UKALLR3: induction, IT methotrexate/dexamethasone oral/mitoxantrone IV or idarubicin IV/vincristine IV/pegaspargase IM; consolidation, dexamethasone oral/vincristine IV/IT methotrexate/methotrexate IV/pegaspargase IM/cyclophosphamide IV/etoposide IV; maintenance, IT methotrexate/dexamethasone oral/vincristine IV/cytarabine IV/Erwinase IM/methotrexate IV; before HSCT, fludarabine IV/cytarabine IV/liposomal daunorubicin citrate IV.5,6
ALL, acute lymphoblastic leukemia; BM, bone marrow; CD, cluster of differentiation; CI, confidence interval; EM, extramedullary; HR, hazard ratio; HSCT, allogeneic hematopoietic stem cell transplantation; iBM, isolated bone marrow; iEM, isolated extramedullary; IM, intramuscular; IT, intrathecal; IV, intravenous; MRD, measurable or minimal residual disease; Ph(–), Philadelphia chromosome–negative; USPI, United States Prescribing Information.
*Patients who had an iBM or combined BM + EM relapse < 36 months or who had an iEM relapse < 18 months were assigned to the high-risk group.5
†Patients who had an iBM or combined BM + EM relapse ≥ 36 months or who had an iEM relapse ≥ 18 months and MRD ≥ 0.1% at end of induction were assigned to the intermediate-risk group.5
COG, Children's Oncology Group; DFS, disease-free survival; HSCT, hematopoietic stem cell transplantation; OS, overall survival; IT, intrathecal.
MRD response after cycle 1 of BLINCYTO® vs block 2 of chemotherapy5,*
MRD
response rate†
75%
(n=79/105)
of patients who received BLINCYTO® achieved MRD negativity vs 32% (n=33/103) of patients who received chemotherapy‡
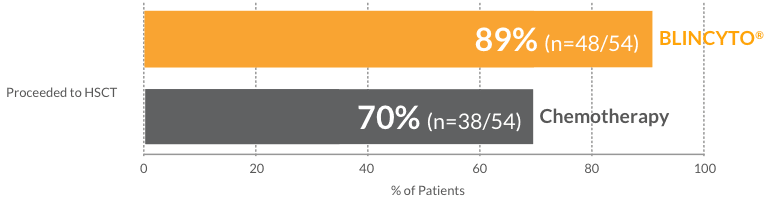
More patients who received BLINCYTO® proceeded to HSCT vs those who received chemotherapy5
*All patients received one block of chemotherapy prior to randomization. Data reflect MRD response for patients who received the first cycle of BLINCYTO® in the BLINCYTO® treatment arm vs patients who received the second block of chemotherapy in the chemotherapy treatment arm.5
†MRD < 0.01%, evaluated in a central laboratory by flow cytometry.5
‡In this analysis, positive MRD or no MRD data are considered as not having negative MRD. The rationale for including patients with no MRD data is that the lack of MRD data was due to death, relapse, or removal from protocol therapy because of an AE or other poor response to therapy, so it is appropriate to include them as the converse of the optimal outcome of being able to submit a sample and have negative MRD.5
Disease-free survival
Overall survival
MRD response
MRD response
Overall survival
Ability to proceed to HSCT
| Key inclusion criteria5 |
|---|
| B-cell precursor ALL in first relapse |
| Key exclusion criteria5 |
| Down syndrome |
| Ph(+) B-cell precursor ALL |
| Previous HSCT or BLINCYTO® treatment |
Baseline characteristics5
| BLINCYTO ® (n=105) n (%) |
Chemotherapy (n=103) n (%) |
|
| Age at enrollment (years) Median (interquartile range) |
9 (6–16) | 9 (5–16) |
| 1–9 | 55 (52.4) | 55 (53.4) |
| 10–12 | 10 (9.5) | 11 (10.7) |
| 13–17 | 25 (23.8) | 19 (18.4) |
| 18–20 | 8 (7.6) | 10 (9.7) |
| 21–27 | 7 (6.7) | 8 (7.8) |
| Sex | ||
| Female | 48 (45.7) | 49 (47.6) |
| Male | 57 (54.3) | 54 (52.4) |
| Risk group assignment after reinduction | ||
| High risk* | 69 (65.7) | 69 (67.0) |
| Intermediate risk† | 36 (34.3) | 34 (33.0) |
| Cytogenetic group at diagnosis | ||
| Favorable ETV6-RUNX1, No. Hyperdiploid with +4, +10, No. |
21 (23.3) 12 9 |
16 (17.6) 8 8 |
| Unfavorable KMT2A-rearranged, No. Hyperdiploid, No. |
7 (7.8) 7 0 |
10 (11.0) 9 1 |
| Other Unknown, No. |
62 (68.9) 15 |
65 (71.4) 12 |
*Patients who had an iBM or combined BM + EM relapse < 36 months or who had an iEM relapse < 18 months were assigned to the high-risk group.5
†Patients who had an iBM or combined BM + EM relapse ≥ 36 months or who had an iEM relapse ≥ 18 months and MRD ≥ 0.1% at end of induction were assigned to the intermediate-risk group.5
‡A low-risk randomization arm was also part of the study.5
§UKALLR3: induction, IT methotrexate/dexamethasone oral/mitoxantrone IV or idarubicin IV/vincristine IV/pegaspargase IM; consolidation, dexamethasone oral/vincristine IV/IT methotrexate/methotrexate IV/pegaspargase IM/cyclophosphamide IV/etoposide IV; maintenance, IT methotrexate/dexamethasone oral/vincristine IV/cytarabine IV/Erwinase IM/methotrexate IV; before HSCT, fludarabine IV/cytarabine IV/liposomal daunorubicin citrate IV.5
HR, high risk; IR, intermediate risk; Ph(+), Philadelphia chromosome–positive.
See the safety results of BLINCYTO® vs chemotherapy in COG AALL1331
Learn moreStudy design: International, open-label, single-arm, phase 1/2 study of single-agent BLINCYTO® in patients < 18 years of age with > 25% BM blasts who were primary refractory, in first relapse after full salvage induction, in second or later relapse, or in any relapse after HSCT. Primary endpoint was CR/CRh* in first 2 cycles: 33% (n=23/70); (95% CI: 22.1–45.1).1,2
Within the First Two Treatment Cycles of BLINCYTO®


| Key inclusion criteria2 |
|---|
| Primary refractory disease |
| First relapse after full salvage induction |
| Second or later relapse, or in any relapse after HSCT |
| Age < 18 years |
| KPS ≥ 50% or LPS ≥ 50% for patients < 16 years of age |
| Key exclusion criteria2 |
| Active acute or extensive chronic GvHD after HSCT |
| Evidence of active CNS involvement |
| Evidence of active testicular involvement |
Baseline Characteristics (N=70)2,*
| Sex, n (%) | |
|---|---|
| Male | 47 (67) |
| Age, n (%) | |
| < 2 years | 10 (14) |
| 2–6 years | 20 (29) |
| 7–17 years | 40 (57) |
| Previous relapses, n (%) | |
| 0 (primary refractory disease) | 2 (3) |
| 1 | 31 (44) |
| 2 | 29 (41) |
| ≥ 3 | 8 (11) |
| Previous HSCT, n (%) | 40 (57) |
| Baseline BM blasts, n (%) | |
| < 50% | 18 (26) |
| ≥ 50% | 52 (74) |
BLAST, the pivotal study of BLINCYTO® in adult patients with MRD(+) B-cell precursor ALL: N=86, an open-label, single-arm phase 2 study of adult patients with MRD(+) B-cell precursor ALL who had received at least 3 chemotherapy blocks of standard ALL therapy, were in hematologic complete remission (defined as < 5% blasts in bone marrow, absolute neutrophil count > 1 Gi/L, platelets > 100 Gi/L), and had MRD* at a level of ≥ 0.1% using an assay with a minimum sensitivity of 0.01%. Primary endpoint: 81% (n=70/86) of patients had no detectable MRD assessed after 1 treatment cycle with BLINCYTO®1,8,*
*Defined as the absence of detectable MRD confirmed in an assay with minimum sensitivity of 0.01% for 6 patients and ≤ 0.005% for 80 patients. Undetectable MRD was achieved by 65 of 80 patients with an assay sensitivity of at least 0.005%.1
†Most patients (n=12) received a single 4-week course of BLINCYTO® at 15 mcg/m2/day; 2 patients had their initial cycle of BLINCYTO® shortened to start HSCT preparative therapy (at days 18 and 20), and 1 patient received 2 courses for a total of 66 days.9
‡Defined as < 5% blasts in the bone marrow.9
§The threshold for MRD positivity may vary based on the protocol being followed and/or the assay being used.11


MRD(+) and R/R: The NCCN Guidelines for Pediatric ALL recommend blinatumomab (BLINCYTO®) as a treatment option for pediatric patients with B-cell precursor ALL in first relapse and those who test MRD(+)§ in first or second complete remission11
WARNING: CYTOKINE RELEASE SYNDROME and NEUROLOGICAL TOXICITIES including IMMUNE EFFECTOR CELL-ASSOCIATED NEUROTOXICITY SYNDROME
BLINCYTO® is contraindicated in patients with a known hypersensitivity to blinatumomab or to any component of the product formulation.
The incidence of signs and symptoms consistent with ICANS in clinical trials was 7.5%. The onset of ICANS can be concurrent with CRS, following resolution of CRS, or in the absence of CRS. Monitor patients for signs or symptoms of neurological toxicities, including ICANS, and interrupt or discontinue BLINCYTO® as outlined in the PI.
Use the preservative-free preparations of BLINCYTO® where possible in neonates. When prescribing BLINCYTO® (with preservative) for neonatal patients, consider the combined daily metabolic load of benzyl alcohol from all sources including BLINCYTO® (with preservative), other products containing benzyl alcohol or other excipients (e.g., ethanol, propylene glycol) which compete with benzyl alcohol for the same metabolic pathway.
Monitor neonatal patients receiving BLINCYTO® (with preservative) for new or worsening metabolic acidosis. The minimum amount of benzyl
alcohol at which serious adverse reactions may occur in neonates is not known. The BLINCYTO® 7-Day bag (with preservative) contains 7.4 mg of benzyl alcohol per mL.
Please see BLINCYTO® full Prescribing Information, including BOXED WARNINGS.
BLINCYTO® is a registered trademark of Amgen Inc.
References: 1. BLINCYTO® (blinatumomab) prescribing information, Amgen. 2. von Stackelberg A, Locatelli F, Zugmaier G, et al. Phase I/phase II study of blinatumomab in pediatric patients with relapsed/refractory acute lymphoblastic leukemia. J Clin Oncol. 2016;34:4381-4389. 3. Locatelli F, Zugmaier G, Rizzari C, et al. Effect of blinatumomab vs chemotherapy on event-free survival among children with high-risk first-relapse B-cell acute lymphoblastic leukemia: a randomized clinical trial. JAMA. 2021;325:843-854. 4. Data on file, Amgen; 2020. 5. Brown PA, Ji L, Xu X, et al. Effect of postreinduction therapy consolidation with blinatumomab vs chemotherapy on disease-free survival in children, adolescents, and young adults with first relapse of B-cell acute lymphoblastic leukemia: a randomized clinical trial. JAMA. 2021;325:833-842. 6. Parker C, Waters R, Leighton C, et al. Effect of mitoxantrone on outcome of children with first relapse of acute lymphoblastic leukaemia (ALL R3): an open-label randomized trial. Lancet. 2010;376:2009-2017. 7. Hogan LE, Brown PA, Ji L, et al. Children's Oncology Group AALL1331: Phase III trial of blinatumomab in children, adolescents, and young adults with low-risk B-cell ALL in first relapse. J Clin Oncol. 2023. doi:10.1200/JCO.22.02200. 8. Gökbuget N, Dombret H, Bonifacio M, et al. Blinatumomab for minimal residual disease in adults with B-cell precursor acute lymphoblastic leukemia. Blood. 2018;131:1522-1531. 9. Keating AK, Gossai N, Phillips CL, et al. Reducing minimal residual disease with blinatumomab prior to HCT for pediatric patients with acute lymphoblastic leukemia. Blood Adv. 2019;3:1926-1929. 10. ClinicalTrials.gov. https://classic.clinicaltrials.gov/ct2/results?term=blinatumomab&cond=Residual+Disease%2C+Minimal&recrs=b&recrs=a&recrs=f&recrs=d&age_v=&gndr=&type=Intr&rslt=&Search=Apply. Accessed July 24, 2023. 11. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Pediatric Acute Lymphoblastic Leukemia v.2.2023. ©National Comprehensive Cancer Network, Inc. 2023. All rights reserved. Accessed March 13, 2023. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
WARNING: CYTOKINE RELEASE SYNDROME and
NEUROLOGICAL TOXICITIES including IMMUNE EFFECTOR CELL-ASSOCIATED
NEUROTOXICITY SYNDROME